The Evolving Science of Omega-3s and Pregnancy
Over the past several years, the connection between omega-3 fatty acids and preterm birth has gained significant scientific support. A landmark Cochrane Review published in 2018 concluded that:
“Omega-3 supplementation during pregnancy is a simple and effective way to reduce preterm, early preterm birth, and low birthweight, with low cost and little indication of harm.”
The researchers even emphasized that more placebo-controlled studies were unnecessary. Yet, in September of the following year, the ORIP trial, published in the New England Journal of Medicine, appeared to challenge that conclusion—showing no benefit and even suggesting potential harm from DHA supplementation.
Reanalyzing the ORIP Trial: A Nuanced Perspective
A new analysis, published in the British Journal of Obstetrics & Gynecology, has offered a more refined understanding of the ORIP results—especially regarding DHA blood levels and the timing of supplementation.
The key insight: the effectiveness of DHA supplementation depends on an individual woman’s omega-3 status. Women who already had sufficient DHA levels at the start of pregnancy did not benefit, and in some cases, may have experienced increased risk with high-dose supplementation. Conversely, women with low DHA status experienced significant protection against early preterm birth when supplementing with omega-3.
What Does This Mean?
-
Personalized DHA testing is the most rational and evidence-based method for determining supplementation needs.
-
Supplementation should be targeted based on DHA blood levels, rather than using a one-size-fits-all approach.
Why Personalization Matters
The concept of personalized medicine isn't new. As noted in a 1999 Newsweek article:
“The cookbook approach to prescriptions defies both medical science and common sense... People respond very differently to medications depending on weight, age, and inborn ability to process drugs.”
This logic extends to omega-3s like DHA and EPA. While dosage matters, identifying individual need and response is critical for determining an effective intake strategy.
Revisiting the ORIP Trial Findings
The ORIP trial (Omega-3 fats to Reduce the Incidence of Prematurity) involved over 5,400 Australian women—making it the largest clinical trial of omega-3 supplementation during pregnancy to date. The original results showed:
-
No effect of DHA supplementation on early preterm birth (before 34 weeks), especially among women who already consumed adequate DHA.
However, an exploratory follow-up analysis, led by Dr. Maria Makrides, provided deeper insight. It revealed that:
-
Women with low omega-3 status in early pregnancy were most likely to benefit from omega-3 supplementation.
-
Women with high omega-3 status at baseline showed no benefit and potentially increased risk.
DHA Thresholds: What the Data Suggest
According to the authors:
“Supplementation may be a useful strategy for women with omega-3 status below 4.1% of total fatty acids at the end of the first trimester.”
This supports blood testing as the most precise method to determine whether DHA supplementation is warranted.
Regarding preterm birth (before 37 weeks):
-
The effect of DHA supplementation did not vary significantly by omega-3 status, possibly because supplementation was stopped at 34 weeks. Continuation until delivery might have influenced the outcome.
Important study design note:
-
The original ORIP trial included both singleton and twin pregnancies.
-
The follow-up analysis focused only on singleton births, where findings are less likely to be skewed by naturally higher preterm rates seen in twins.
DHA Expert Commentary: Dr. Kristina Harris Jackson
Dr. Kristina Harris Jackson, a leading expert in prenatal DHA research, commented:
“Higher baseline omega-3 status was associated with lower risk of early preterm birth, but DHA appeared to be the most predictive single fatty acid.”
She highlighted a striking result: Women with low baseline omega-3 status who took 900 mg of DHA reduced their early preterm birth risk by 77% compared to placebo.
Target DHA Levels: Practical Recommendations
Dr. Jackson’s own 2018 study formed the foundation for recommending a target Prenatal DHA blood level of 5%. Based on the ORIP data, she offered the following DHA supplementation guidance:
| Prenatal DHA Level | Recommended Daily DHA Dose |
|---|---|
| < 3% | 800–1000 mg |
| 3–5% | ~200–800 mg (avg ~600 mg) |
| ≥ 5% | Maintain with ~200 mg/day |
Dr. Jackson noted that the estimated median Prenatal DHA level in ORIP was 4.6%, which may be higher than the average U.S. population. In that case, a lower DHA dose (200–600 mg/day) might have been more effective and appropriate.
Global Perspective: Supporting DHA Early in Pregnancy
A January study from Belgium emphasized the importance of establishing healthy omega-3 blood levels early in pregnancy. Researchers advocated for:
-
Personalized nutritional support for pregnant women
-
Routine DHA blood testing to guide dietary and supplement decisions
-
Aiming to reach the 5% target DHA level to reduce risks of adverse pregnancy outcomes like preterm birth
Final Thoughts
The research is clear: omega-3 supplementation during pregnancy can be highly effective—but only when tailored to the individual. Women with low DHA status benefit significantly, while unnecessary high doses may cause harm in those already sufficient.
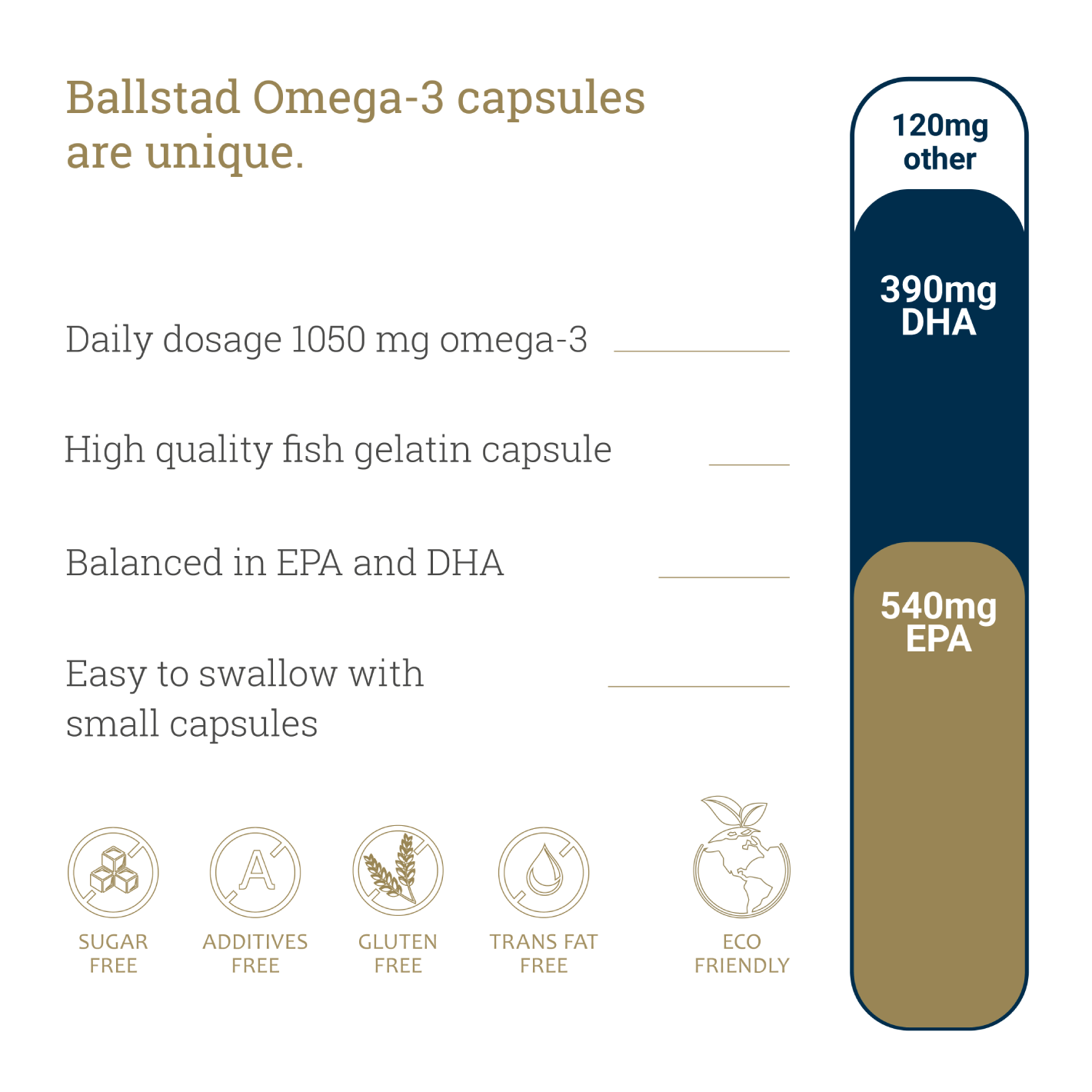
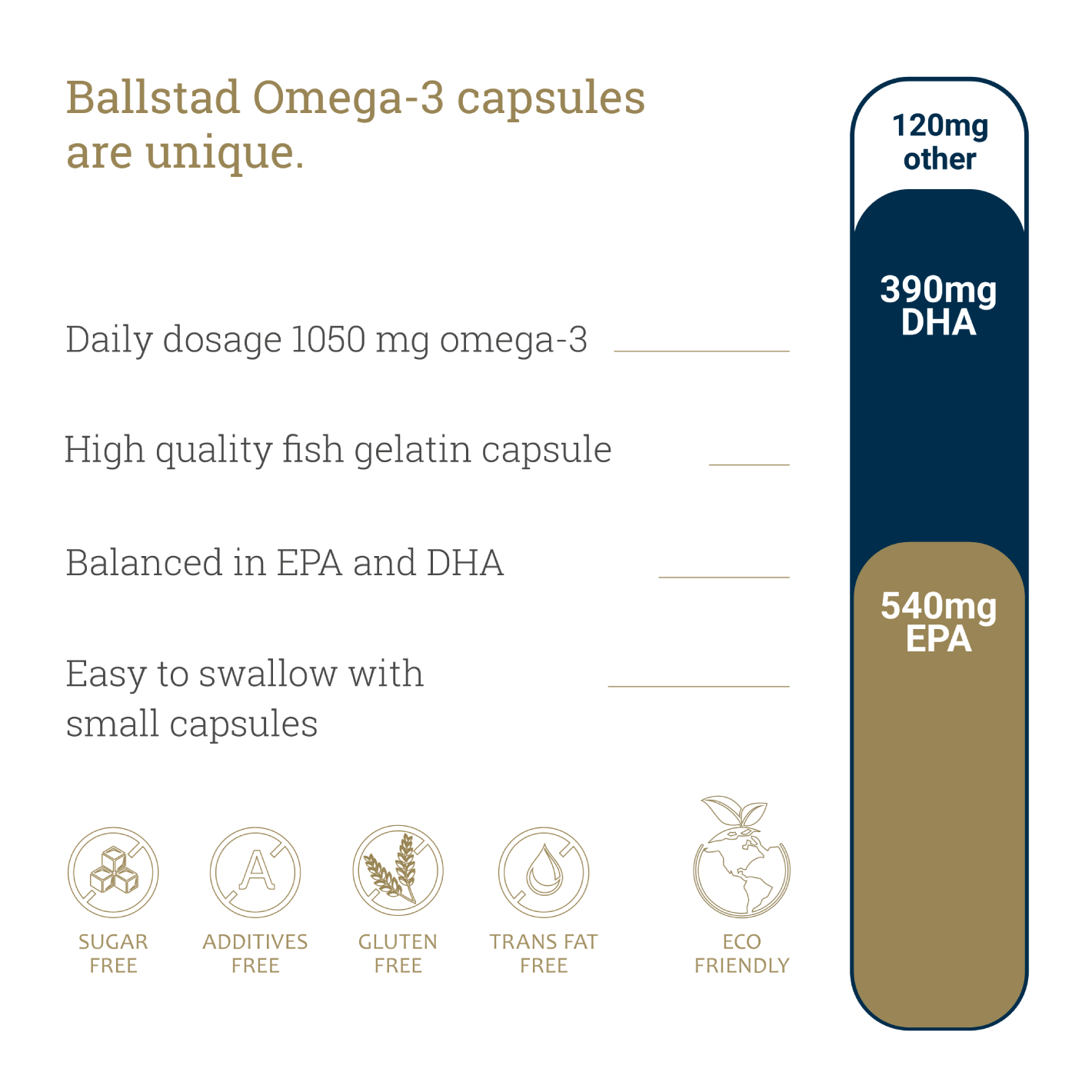
Personalized testing and targeted DHA supplementation offer the safest, most effective path forward. For pregnant women, especially those with limited dietary fish intake, high-quality omega-3 products like Ballstad Omega-3 provide a reliable way to reach optimal DHA levels and reduce the risk of preterm birth.
Credit: OmegaQuant Website